The Science
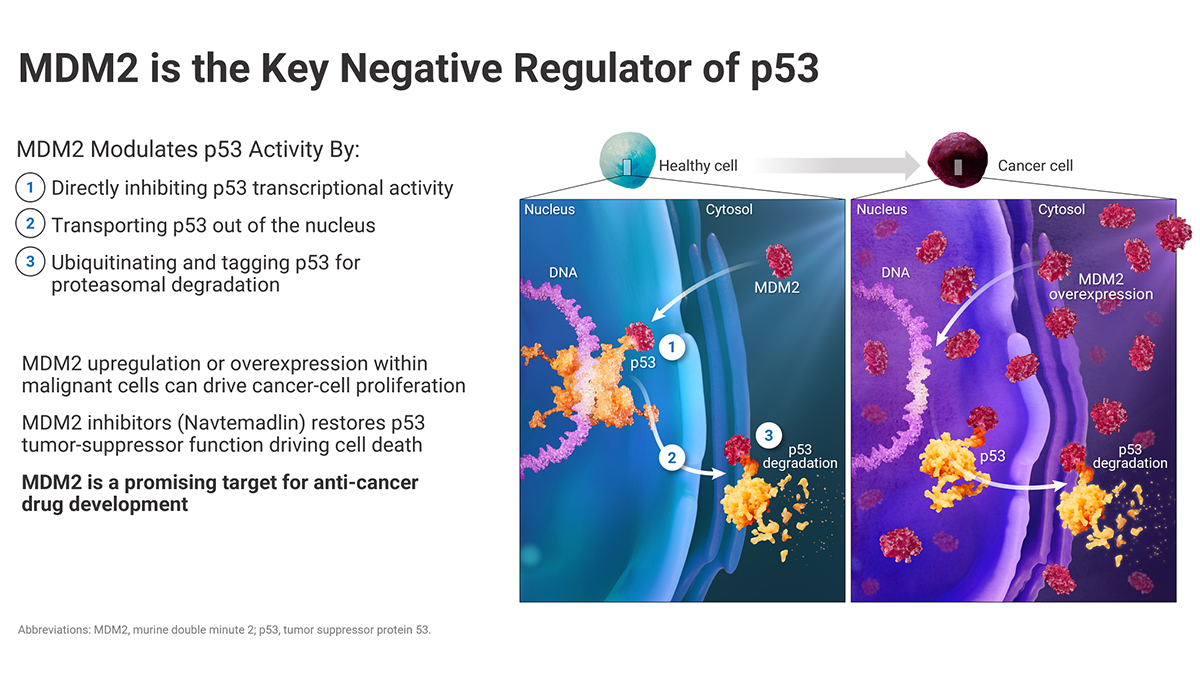
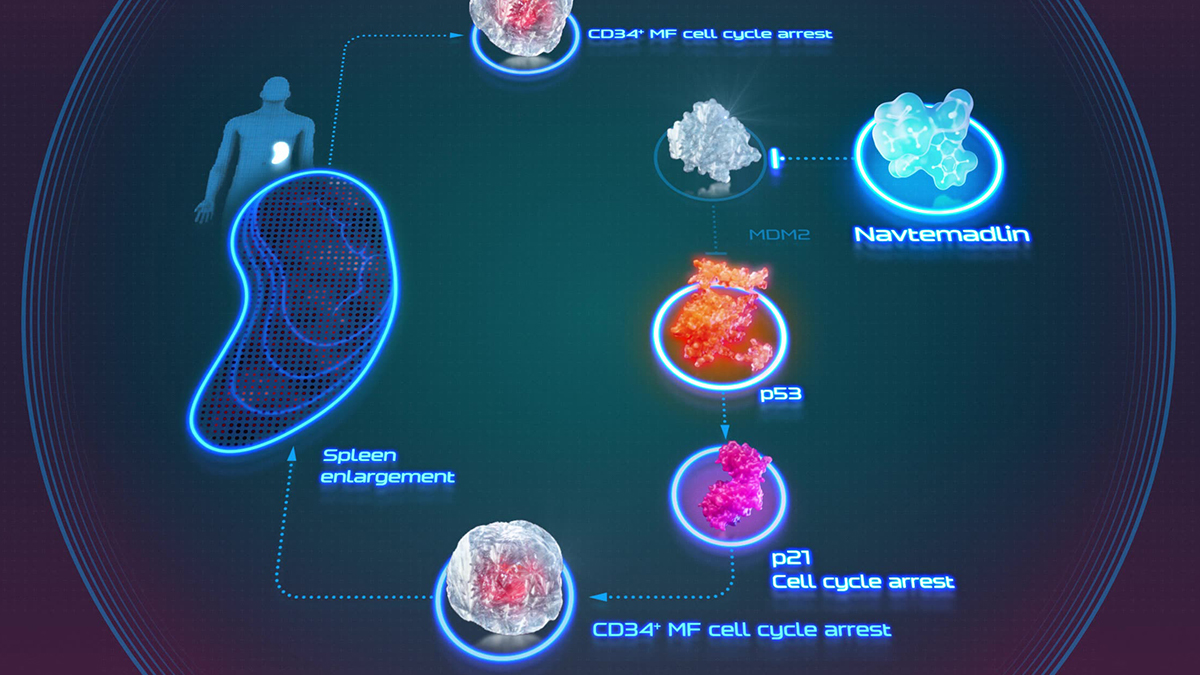
Myelofibrosis begins with a driver mutation that activates JAK/STAT signaling and elevates MDM2, the ligase that marks the tumor suppressor p53 for degradation. The TP53 gene stays intact, but the p53 protein is suppressed and cannot clear the malignant clone.
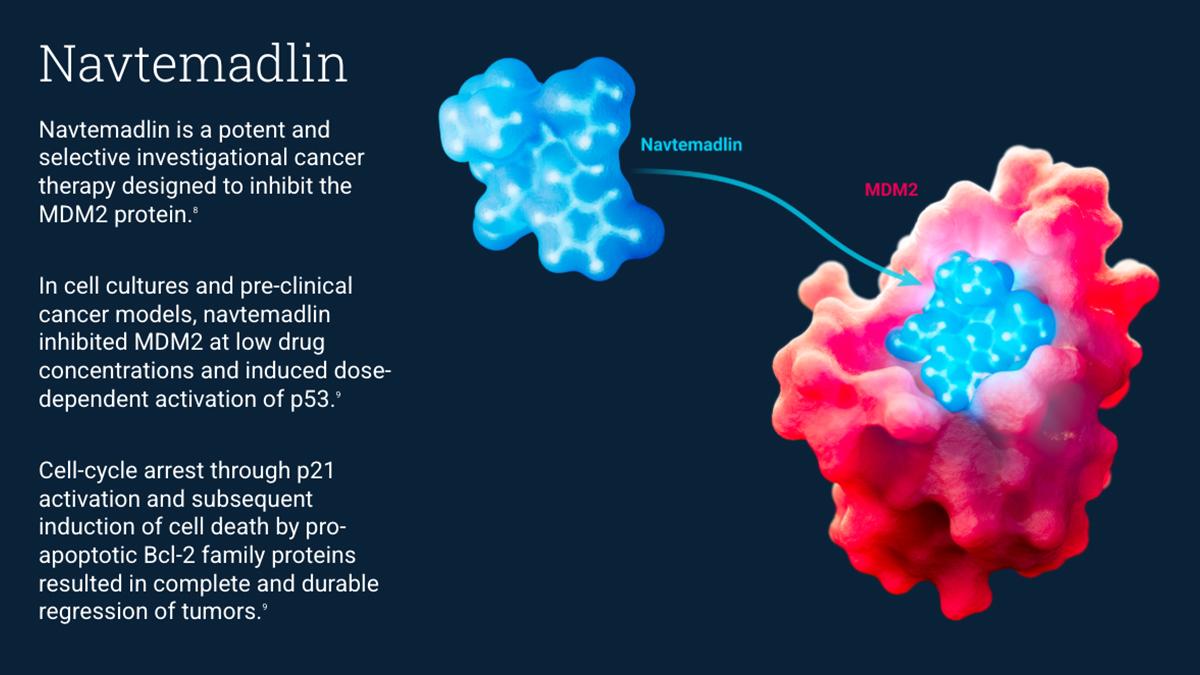
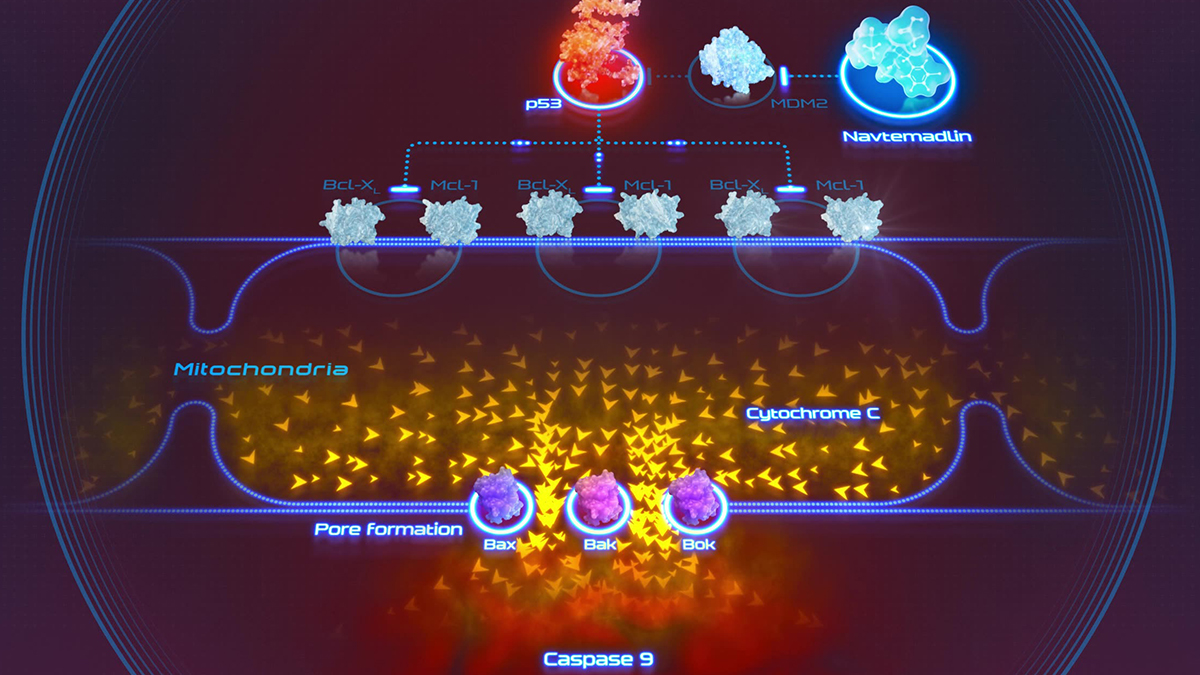
Navtemadlin, a selective oral MDM2 inhibitor, blocks the MDM2–p53 interaction, freeing p53 to drive apoptosis in TP53 wild-type cells through pro-apoptotic BCL-2 modulation. It acts on a node ruxolitinib never reaches, clearing the clone standard treatment leaves behind.
The Challenge
Navtemadlin's problem was not obscurity but doubt.
MDM2 inhibition carried two decades of failure. The rationale was always elegant: reactivate p53 where the gene is intact but suppressed. Turning that biology into a credible drug was where the class kept collapsing. A sophisticated evaluator would ask why this molecule differed from the ones that burned the field before. The answer lived in the mechanism and in dense, biomarker-selected trial data most people cannot read at a glance. To be assessed at its real value, the biology had to be seen, not just described.
The Outcome
Seen clearly, the asset read the way a late-stage program should.
The mechanism differentiated navtemadlin from a class the field had written off. The combination logic, navtemadlin layered on ruxolitinib rather than replacing it, framed a rational new standard. Ipsen acquired Kartos for up to $1.75 billion, making navtemadlin its first hematology asset and a late-stage addition to its oncology pipeline. For the roughly 40% of patients who never respond fully to standard of care, it points to a new option.
Navtemadlin (KRT-232) is investigational and has not been approved by any regulatory agency. Deal terms reflect Ipsen's announced acquisition of Kartos Therapeutics (June 29, 2026).
References
- 1 BOREAS (NCT03662126): Mascarenhas JO, et al. Results from the Randomized, Multicenter, Global Phase 3 BOREAS Study. Blood 2024;144(Suppl 1):1000. SVR35 15% vs 5% (BAT); ~48% bone marrow fibrosis reduction; ~82% mean CD34+ reduction at Week 24.
- 2 KRT-232-109 (NCT04485260): Mascarenhas J, et al. Phase 1b/2 add-on study, navtemadlin plus ruxolitinib. HemaSphere 2023 (EHA 2023): SVR35 and TSS50 each 32% at Week 24.
- 3 POIESIS (NCT06479135; EUCT 2023-504724-25-00): Vachhani P, et al. Future Oncology 2026;22(7):781–793. Registrational Phase 3 add-on design; co-primary SVR35 and TSS50 at 24 weeks; top-line expected 2027.
- 4 Mechanism: Nakatake M, et al. JAK2 V617F negatively regulates p53 stabilization by enhancing MDM2 via La expression in myeloproliferative neoplasms. Oncogene 2011. Review: MDM2 inhibitors in myeloid cancers. Leukemia 2026.
- 5 Deal: Ipsen to acquire Kartos Therapeutics, June 29, 2026 ($450M upfront; up to $1.3B milestones; up to $1.75B total; expected close end of Q3 2026).