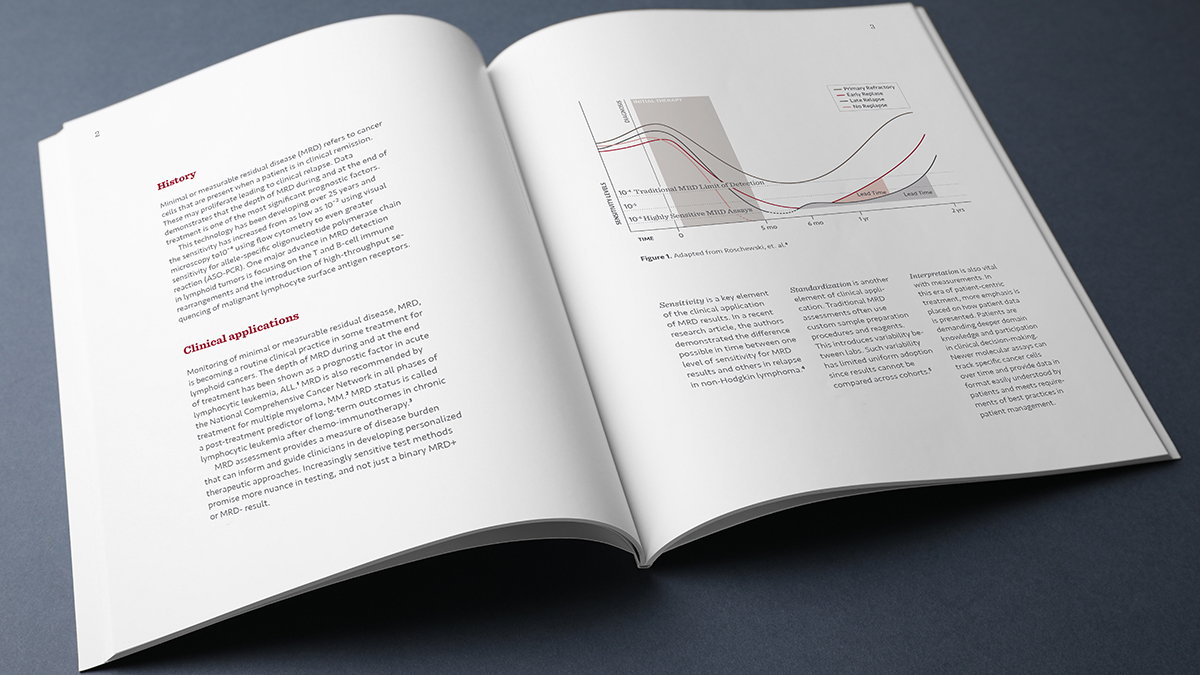
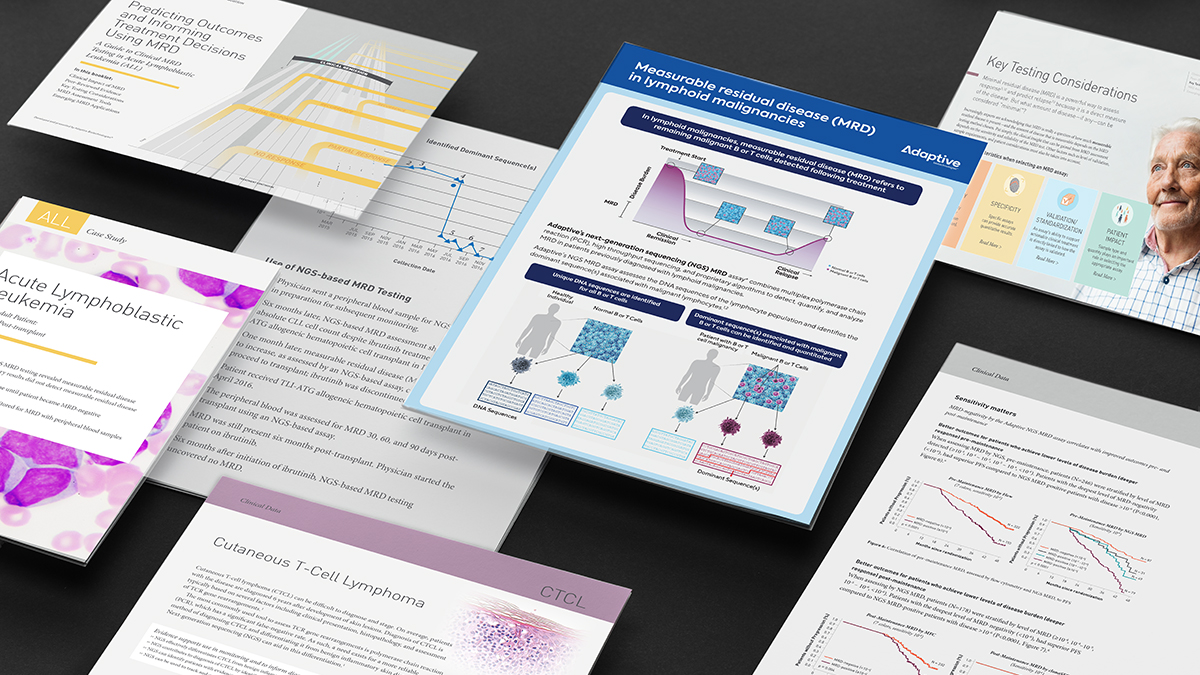
The Science
MRD is the small population of cancer cells that survives treatment, below the detection limit of standard response assessment. clonoSEQ uses multiplex PCR and next-generation sequencing to identify the DNA signature of a patient's malignant clone at diagnosis, then tracks those exact sequences in later samples, detecting one cancer cell among a million.
It reframes what response means: not whether disease is visible, but how much remains. In 2018 it became the first FDA-cleared NGS MRD assay for any lymphoid cancer.
The Challenge
The science was sound; the belief wasn't there.
In 2018, physician research found limited belief that MRD was clinically actionable — many community hematologists didn't know the term, and even MRD testers couldn't say how a result should change a decision. MRD faced the classic new-category trap: guidelines lagged, reimbursement lagged, and clinicians defaulted to the tests they knew. For a first-in-class diagnostic, the barrier wasn't proving the assay worked. It was making an entire field understand what MRD was, believe it mattered, and know what to do with it.
The Outcome
Education didn't make the science true. It made the science adoptable.
The category the unbranded program was built to establish took hold. MRD moved from an acronym community physicians didn't recognize to a concept embedded in NCCN and ELN guidelines and reimbursed by Medicare across multiple malignancies. The belief that was missing in 2018 — that MRD is clinically actionable — became the field's default.
Cognition built the unbranded education system that made the category legible; guideline, reimbursement and regulatory milestones are the field's, driven by many contributors alongside the science.